This year, the World Health Day is dedicated to maternal and newborn health, supported by the WHO :
“Good health at birth for a hopeful future”.
A major issue that the cardio-pediatrics department addresses on a daily basis. Screening, diagnosis, therapeutics and medico-surgical and interventional management, the identification of genetic factors of congenital heart disease are at the heart of his daily actions.
Professor Sylvie DI FILIPPO has chosen to intervene on the social networks of the Center, in 3 distinct themes (click on the titles to access the videos):
Roca Team captain Yakuba Ouattara has always been committed to helping sick and underprivileged children, and for the past 3 years he has been the patron of the No Finish Line, Monaco’s biggest charity race.
He came to see 7-year-old Aziz, who was operated on by the paediatric cardio team at Monaco’s Cardio-Thoracic Centre, which is very involved in humanitarian work since its creation. This little Ivorian suffered from a serious heart defect that could not be treated in his country of origin.
The operation was made possible thanks to the involvement and generosity of Children & Future, the Department of International Cooperation, the MCH, the Monegasque Red Cross, Aviation sans Frontières and Aziz’s host families.
Giving a second life to sick children from developing countries is a strong commitment from the Principality and one that mobilises this sportsman with a big heart!
Pr. Sylvie DI FILIPPO Monaco Cardiothoracic Center.
Pediatric and adult congenital cardiology & fetal cardiology.
University professor, hospital practitioner.
Congenital heart disease is the most common congenital organ anomaly. Their incidence in the general population is 14 foetuses per 1000 and 8 births per 1000.
Congenital heart disease includes multiple malformations of varying anatomical and functional complexity and with heterogeneous prognoses.
These malformations are classified according to their severity and complexity into:
Minor, moderate and major
Repairable and non-repairable
Biventricular and univentricular
Cyanogenic and non-cyanogenic
Minor heart disease
No need for intervention
Moderate heart disease
Intervention indicated
Repairable heart disease
Severe heart disease
Heart disease requiring treatment and intervention
Repairable with sequelae or non-repairable
Bicuspid aortic valve
Small atrial septal defect
Small interventricular septal defect
Small ductus arteriosus
Minor mitral valve anomaly
Minor pulmonary narrowing
Pulmonary vein anomalies
Coronary anomalies
Aortic stenosis
Atrioventricular canal
Large AIC
Large IVC
Large ductus arteriosus
Aortic coarctation
Tight pulmonary stenosis
Marfan’s disease and aortic aneurysm
Ebstein’s tricuspid anomaly
Tetralogy of Fallot
Transposition of large vessels after repair
Heart disease with fixed pulmonary hypertension (Eisenmenger)
Non-operated or palliated cyanotic heart disease
Interruption of the aortic arch
Right ventricle with double outlet
Single ventricles
Pulmonary atresia
Common arterial trunk
Univentricular Fontan circulation
Transposition of the great vessels with right ventricle under the aorta
Complex heart disease with multiple lesions
Anatomo-physiopathological classification of congenital heart disease
Left-right shunts
Right-to-left shunts and right obstructions
Left obstructions
Coronary anomalies
Rhythmological abnormalities
Complex heart disease
Shunt: natural or created abnormal communication between heart chambers or vessels.
Cyanosis: blue discolouration of the skin and mucous membranes due to a drop in oxygen in the blood (or hypoxia).
Antenatal screening
Congenital heart disease is well tolerated during intrauterine life and does not prevent normal development of the foetus.
Adaptation to extra-uterine life, which involves a fall in pulmonary pressures and closure of the ductus arteriosus and foramen ovale, is the cause of decompensation of cardiac malformations, the viability of which depends on the permeability of these shunts.
Antenatal diagnosis of heart disease by echocardiography and Doppler enables decompensation to be anticipated and prevented, by guiding immediate post-natal therapeutic management. The birth is programmed and planned by the gynaeco-obstetric and neonatology team.
In the majority of cases, pre-term induction is not necessary. Only cases of fetal heart failure may justify it (the consequence of an abnormal heart rhythm, either too slow = fetal bradycardia, or too fast = uncontrolled fetal tachycardia).
Antenatal screening enables heart disease to be diagnosed, with results ranging from 40% to 90% depending on the type of heart disease.
It enables a diagnosis to be made, the course of the disease to be monitored antenatally, postnatal care to be planned and the prognosis to be established.
Birth planned in this way helps prevent decompensation of the heart disease after birth
The prostaglandin E1 administered is a treatment that keeps the ductus arteriosus open at birth, thereby maintaining circulation and/or oxygenation in newborns with heart disease at risk of acute decompensation.
Heart diseases at risk of neonatal decompensation entail a lethal risk, including::
– Right-sided obstructions that limit pulmonary flow
– Left-sided obstructions that limit aortic flow
– Mixing anomalies that depend on the patency of the foramen ovale
Diagnosis and clinical symptoms
Newborn
Cyanosis, heart failure
Shunt-dependent heart disease
Symptoms
Feeding difficulties
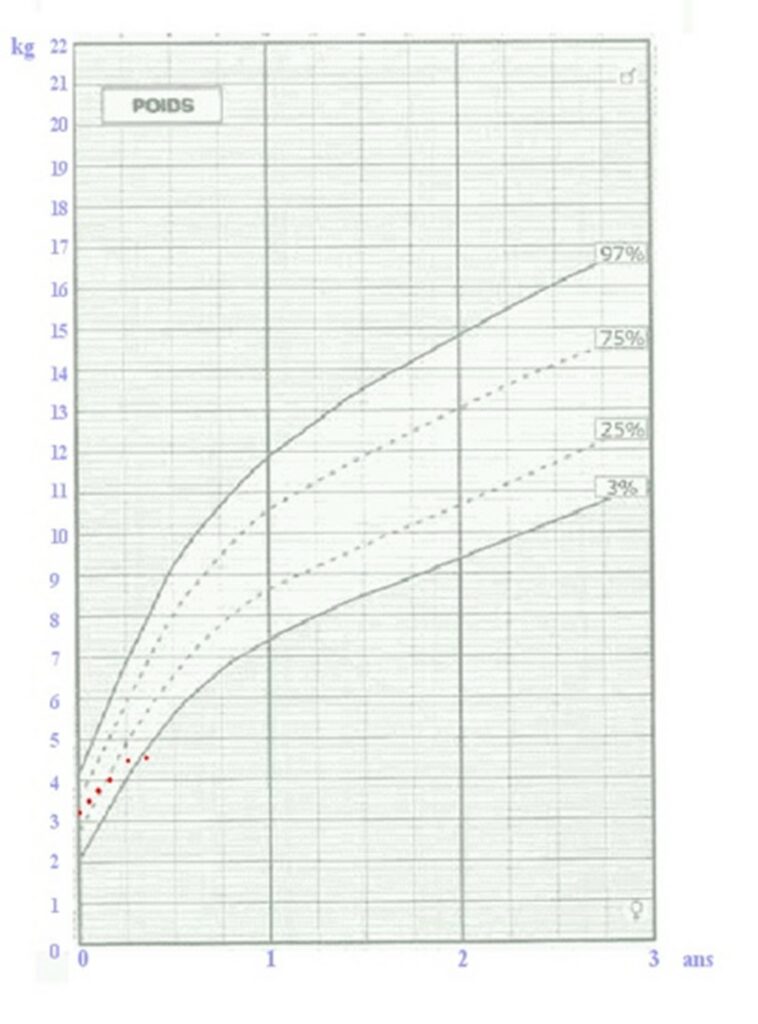
Poor growth or weight stagnation
Frequent bronchopulmonary infections
Dyspnoea on exertion
Feeling unwell, syncope
Chest pain
Asymptomatic
Breathing
ECG abnormality discovered by chance
Abnormalities on clinical examination: femoral pulses, high blood pressure
Auscultation: detection of a murmurInfant weight growth curve: weight stagnation (red dots)
Cardiac and Doppler ultrasound: cardiac ultrasound is a simple, non-invasive examination that can be used to diagnose cardiac malformations at any age.
Neonatology
Screening for congenital heart disease
Antenatal
heart disease detected antenatally must be confirmed postnatally by a cardiac ultrasound scan of the newborn.
Postnatally
not all heart disease is detected before birth, and it is still very important to examine all newborn babies in the maternity unit to look for any heart abnormality that may have gone unrecognised, and to recognise it before the baby is discharged home.
The clinical examination should look for :
palpation of the femoral pulses
The presence of a murmur on ausculation
The newborn’s feeding behaviour
Oxygen saturation or satO2: systematic screening for heart disease in newborns is carried out in maternity units by measuring oxygen saturation in the upper and lower limbs. The normal level is > 97%, with a difference of less than 3% between the upper and lower limbs. If this measurement is abnormal, an echocardiogram is performed to check for any cardiac abnormality before the baby is discharged from the maternity hospital.
Saturation sensor
Imaging congenital heart disease
IRM
Magnetic resonance imaging makes a major contribution to the assessment of congenital heart disease, particularly in adulthood, when the performance of echocardiography is less good. MRI provides additional information that is essential for assessment, follow-up, diagnosis, management and therapeutic decisions. It allows :
Anatomical assessment of cavities and vessels
Functional assessment: of myocardial function
Analysis of flow and output
Search for myocardial fibrosis
Testing for ischaemia using the adenosine test
Its use is limited in children because of the need for sedation
The main indications are systemic right ventricles (double mismatch, transposition of the great vessels with atrial switch), right ventricles with volume overload (tetralogy of Fallot), single ventricles, pulmonary, aortic, tricuspid and mitral valve disease, aortic pathologies, etc.
SCANNER
The angio-scanner is a complementary imaging technique which allows the vessels to be viewed in particular:
pulmonary arteries
pulmonary veins
coronary arteries
aorta
veno-venous and arteriovenous fistulas
Its use is limited by irradiation and injection of potentially nephrotoxic and allergenic contrast medium.
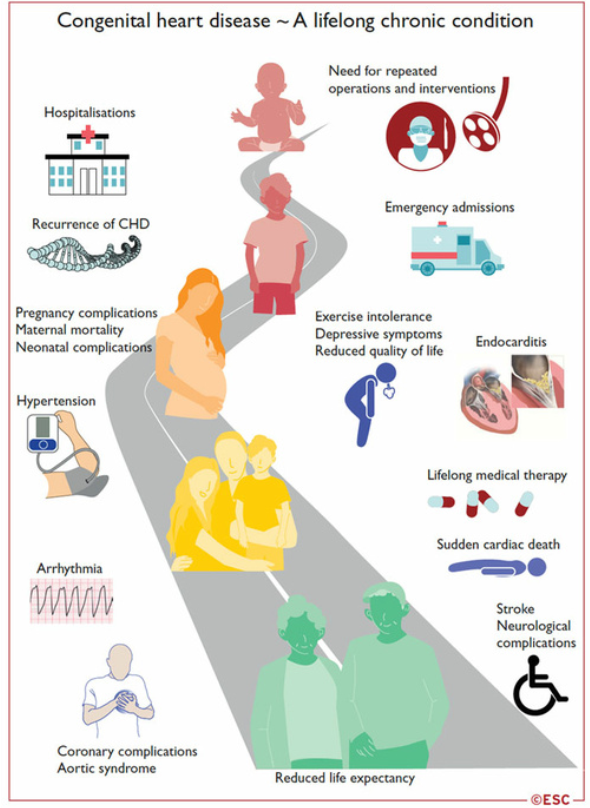
Congenital heart disease in adulthood
Over 90% of children with congenital heart disease (CHD) survive into adulthood.
The number of adults with CHD is now greater than the number of children.
Most of these patients cannot be considered cured, and their management is a lifelong process: from repair in childhood, to the transition to adulthood, to the desire for pregnancy, and the management of late complications specific to each CC.
ESC 2020 recommendations: management of congenital heart disease in adulthood.
Transition to adulthood
The transition to adulthood is an important phase that needs to be anticipated and supported, so that patients can receive all the information they need about their heart disease, their medical history, their treatment, their follow-up and all the problems associated with their heart disease.
To this end, therapeutic education programmes have been developed and set up in the referral centres.
At the CCM: the transition is made naturally by an organisation based on a medical-surgical team caring for the same patients from foetus to adulthood.
Complications of congenital heart disease in adulthood:
Myocardial dysfunction: left ventricle, single ventricle, systemic right ventricle
Coronary artery disease
Heart failure
Arrhythmias
Infectious endocarditis
Arterial hypertension
Transmission and genetics of congenital heart disease
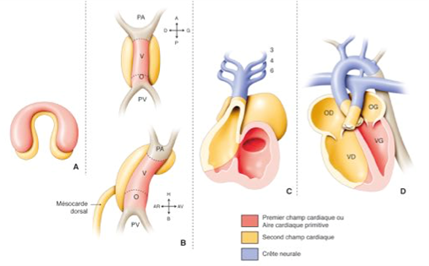
Embryology of the normal heart: the heart is formed during the first 8 weeks of foetal life, in several successive complex stages starting from the primitive cardiac tube, with phenomena of torsion and rotation and partitioning:
Primitive heart tube
Loop: position of the atria/ventricles cavities
Formation of the atrioventricular valves
Partitioning of the atria
Partitioning of the ventricles
Partitioning of the vessels
Congenital heart disease is inherited through a multifactorial mechanism involving both genetic and environmental factors.
In the majority of cases (72%), no genetic aetiology is identifiable.
Genetic and environmental factors: account for 20% to 30% of cases
Environmental factors: 2% of cases
Maternal illnesses: diabetes, rubella, systemic lupus erythematosus.
Maternal use of treatments such as lithium, isotretinoin and anticonvulsants.
Maternal age: this is a risk factor for trisomy 21, which can lead to heart malformations.
Chromosomal abnormalities (aneuploidies): 10%.
trisomy 21 or Down syndrome, trisomy 18, trisomy 13, monosomy X or Turner syndrome
monogenic: congenital syndromes affecting multiple organs
Di George syndrome (microdeletion 22q11.2)
Williams-Beuren syndrome (microdeletion 7p11.23)
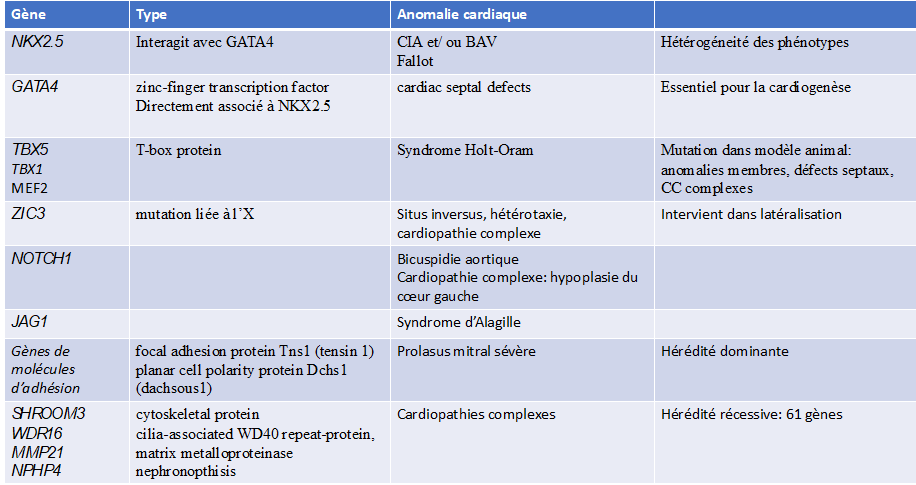
Single gene defects: fibrillin-1 mutations (Marfan syndrome), TXB5 (Holt-Oram syndrome)
PTPN11 (Noonan syndrome).
Autosomal dominant de novo point mutation: 8%.
Autosomal recessive inherited point mutation: 2%.
The risk of recurrence of congenital heart disease in a family depends on the cause: negligible in de novo mutations, 2 to 5% in non-syndromic multifactorial congenital heart disease, and 50% when an autosomal dominant mutation is involved.
It is important to identify genetic factors in order to assess the risk of recurrence and to guide preconception genetic counselling.
Table: examples of genetic mutations with associated heart disease.
How can we help you?
EMERGENCY
Contact +377 92 16 80 00 Emergencies relating to cardiovascular and thoracic pathology are accepted without restriction, 24 hours a day, 7 days a week, Sundays and public holidays included.






 Congenital heart disease is inherited through a multifactorial mechanism involving both genetic and environmental factors.
Congenital heart disease is inherited through a multifactorial mechanism involving both genetic and environmental factors.